
IVDR Article 10 labeling rules: stricter than MDR
- Apr 21
- 8 min read
Experienced IVD manufacturers who assumed their MDR translation workflows would carry over to IVDR have been caught off guard. IVDR Article 10 imposes labeling and language obligations that go beyond what MDR requires, and the gap is not marginal. Device information that was acceptable under MDR may fail notified body scrutiny under IVDR, particularly when translation quality, legibility, and patient-facing clarity are assessed. This guide explains what Article 10 and Annex I Section 20 actually demand, why IVDR raises the bar higher than MDR, and how regulatory affairs and QA managers can build a translation validation process that holds up under audit.
Table of Contents
Key Takeaways
Point | Details |
IVDR labeling is stricter | IVDR Article 10 raises labeling and translation demands well above MDR, increasing regulatory scrutiny for IVD manufacturers. |
Language validation is critical | Manufacturers must ensure all IVD labeling is clear, indelible, and easily understood in each EU country’s official language. |
Non-compliance carries real risks | Labeling or translation errors can lead to corrective actions, regulatory penalties, and market barriers for IVDs. |
Strategic translation adds value | Approaching IVDR translation as more than a checkbox can reduce risk and strengthen brand trust. |
What IVDR Article 10 demands: A closer look at the labeling rules
With that context, it is essential to understand the letter of the law in Article 10 before comparing IVDR and MDR.
IVDR Article 10 mandates that device information be indelible, legible, and provided in the official language or languages of each EU Member State where the device is placed on the market. This is not a soft recommendation. It is a hard obligation tied directly to CE marking and market access.
Annex I Section 20 of the IVDR defines the specific content that must appear on the label and in the instructions for use. This includes the intended purpose, performance characteristics, contraindications, and instructions that enable safe and correct use. Every single element must be rendered accurately in the target language, not approximately, and not in a way that could cause the user to misread a critical instruction.
The phrase easily understandable carries real regulatory weight here. For patient-near and self-test devices, the intended user may not have clinical training. That shifts the translation burden significantly. A label translated for a trained lab technician cannot simply be reused for a home-use glucose monitoring kit. The vocabulary, sentence structure, and layout must all support comprehension for a lay reader.
Indelible also matters more than it might seem. If labeling is printed on packaging that degrades, or if digital labeling systems display inconsistent text across language versions, that creates a compliance gap.
Here are the non-negotiable requirements from Article 10 for labeling and translation:
All labeling must appear in the official language(s) of the Member State(s) where the device is marketed
Language must be easily understandable by the intended user, including lay users for self-test devices
Information must be legible, indelible, and not misleading
Certified IFU translations must meet the requirements of Annex I Section 20
UDI-DI label consistency must be maintained across all language versions submitted to EUDAMED
Translations must be validated and traceable for notified body review
“Manufacturers who treat translation as a final-step formatting task rather than a regulated activity will find Article 10 compliance far harder to demonstrate when a notified body comes asking for documentation.”
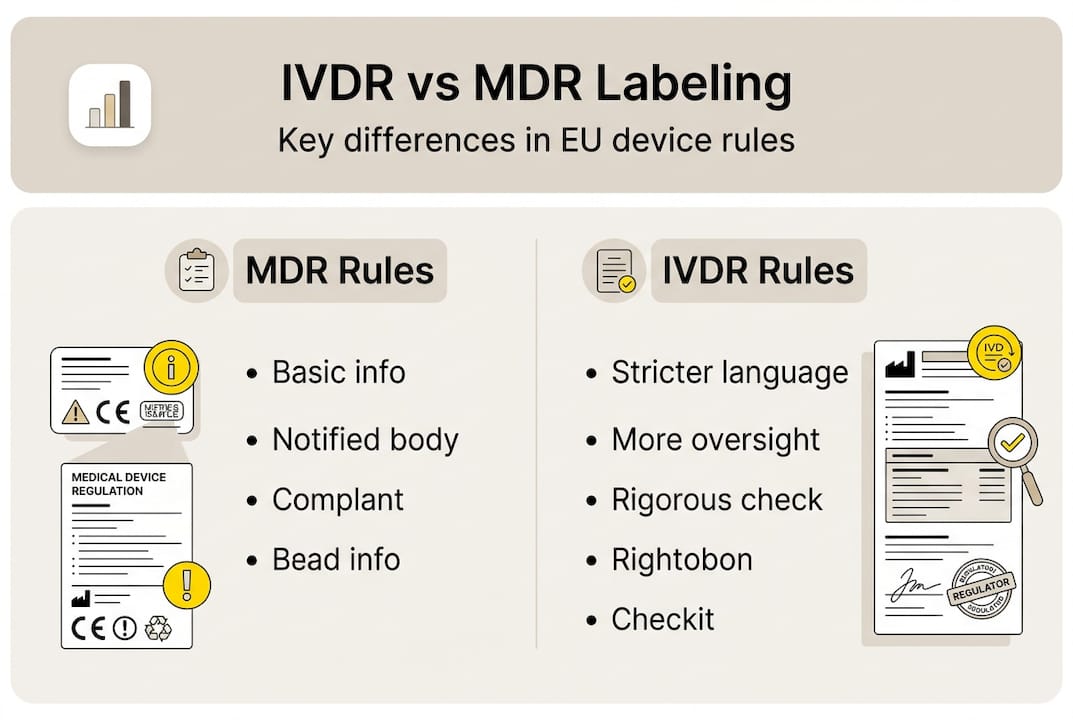
IVDR vs. MDR: Why is IVD labeling regulated more strictly?
Knowing the baseline, we can directly compare how IVDR raises the labeling and translation stakes compared to MDR.
IVDR labeling is stricter due to higher device reclassification rates, expanded UDI mandates, and a much stronger emphasis on clinical performance information on the label itself. Under IVDR, a significant proportion of previously low-risk IVDs have been reclassified into higher risk classes, bringing notified body involvement to a far larger share of the IVD market than before.
Here is a direct comparison of key labeling and translation requirements:
Requirement | MDR | IVDR |
Official language obligation | Yes | Yes, stricter enforcement |
Annex I labeling content | General device info | Clinical performance and self-test clarity |
UDI-DI label consistency | Required | Required plus EUDAMED cross-check |
Patient-facing language standard | User-appropriate | Lay-user comprehension for self-test devices |
Notified body translation review | Selective | More systematic for higher-risk IVDs |
Post-market labeling updates | Required | Required with performance re-evaluation link |
The 80% figure matters here. Under IVDR, the vast majority of IVDs that previously self-certified now require notified body involvement. That means translation packages, language validation records, and label consistency documentation are now subject to formal review rather than internal sign-off alone. Your MDR documentation translation guide experience is a foundation, but it does not substitute for IVDR-specific translation validation.
For self-test and near-patient IVDs, any translation failure carries direct patient risk. A misread instruction on a home coagulation test or an HIV self-test is not an administrative error. It is a safety event.
Pro Tip: Map your device’s risk class under IVDR before assuming your existing MDR translation process applies. Class C and D IVDs face the most intensive notified body scrutiny, and your labeling translation package needs to reflect that with explicit validation evidence.
The translation challenge: From language choice to validation
Having established the stricter regulatory climate, let us look at how IVD translation and language requirements are handled in practice.
IVDR mandates that labeling be easily understandable for intended users, especially for patient-near and self-test devices, which fundamentally changes how translation workflows must be structured. A workflow designed for technical documentation aimed at lab professionals is not fit for purpose when the end user is a patient at home.
Here is a structured translation workflow for IVDR labeling compliance:
Language selection. Identify all Member States where the device will be marketed and confirm the required official language(s) for each, including regional variants where applicable.
Translation brief. Define the intended user profile per language version. A self-test kit translated for German-speaking lay users needs different readability targets than a lab analyzer IFU for Austrian clinical staff.
SME-led translation. Use subject-matter expert linguists with IVD-specific knowledge. General medical translators may not understand performance evaluation terminology or the clinical context of specific analytes.
Back-translation and review. Conduct back-translation from target language to source to catch semantic drift. Pair this with in-country reviewer sign-off.
Readability and comprehension validation. For lay-user devices, run user comprehension checks to confirm the translated label performs as intended with the actual target audience.
UDI-DI consistency check. Confirm that label text submitted to EUDAMED exactly matches the physical label and IFU across all language versions. Inconsistencies here trigger non-conformities.
Notified body submission package. Compile translation validation records, reviewer credentials, comprehension test results, and change history for formal review.
Common QA failures include ambiguous negations (a critical problem in safety warnings), font size or legibility drops when text expands in translation, and terminology inconsistency between the label and the IFU. The medical translation compliance guide covers readability standards in detail, and understanding the risks of unvetted translators is essential before assembling your translation team.
Pro Tip: Build a device-specific term base before translation begins. Lock terminology for analyte names, procedural steps, and safety warnings. This single step eliminates most consistency failures across multilingual label sets.
What non-compliance looks like: Real-world risks and best practices
Now that you know how the translation process works, let us examine what non-compliance means and how leading companies avoid it.
IVDR requires patient-facing labeling to be in national languages and easily understandable, and when that standard is not met, the consequences are concrete. Notified bodies have issued non-approvals based solely on translation quality. Competent authorities in Member States have the power to suspend market access if labeling is found to be misleading or inaccessible to users. Recalls driven by labeling failures are costly in financial terms and damaging in reputational terms.
Real scenarios that have created compliance problems include: a multilingual IFU where the Polish translation omitted a contraindication present in the English source; a self-test device where the French label used clinical terminology flagged as incomprehensible by lay-user testers; and a EUDAMED submission where the UDI-DI label content differed between the English and Spanish versions, triggering a data integrity query.
The most common pitfalls in IVD translation and labeling:
Using translators without IVD domain knowledge
Skipping user comprehension validation for lay-user devices
Failing to maintain UDI-DI label consistency across language versions
Treating translation as a one-time task rather than a controlled, version-tracked process
Not documenting translator credentials and review steps for notified body audit
Overlooking managing multilingual trial risks during device performance studies
Best practice | Process step | Responsible role |
Term base development | Pre-translation | RA Manager + SME linguist |
Back-translation review | Post-translation | Independent SME reviewer |
User comprehension testing | Validation phase | Clinical affairs or UX team |
EUDAMED label consistency audit | Pre-submission | QA Manager |
Translation change control | Post-market | RA + Quality System |
NB submission package | Regulatory filing | RA Manager |
For post-market surveillance translation, label changes triggered by performance data or vigilance reports must flow through the same controlled translation process. A shortcut here is a common source of repeat non-conformities.
Why stricter IVDR labeling is a chance to rethink translation strategy
After seeing the stakes, it is worth rethinking how your organization approaches translation under IVDR.
Many RA and QA teams treat translation as a compliance checkbox. Get it done, file it, move on. That framing creates fragility. When a notified body asks for evidence of comprehension validation or when a competent authority requests your term base and review records, a checkbox approach leaves gaps that are hard to close quickly.
The manufacturers who handle IVDR labeling most confidently are those who invested in translation infrastructure early. They built term bases before their first submission. They ran comprehension checks that generated actual data. They established change control for label text the same way they manage design changes.
Stricter IVDR rules, viewed through that lens, push organizations toward translation practices that reduce long-term regulatory risk and strengthen product reputation in every EU market. A device with clearly validated, user-comprehensible labeling in 20 languages signals quality to regulators and end users alike. Solving translation bottlenecks early in development rather than at submission is where the real competitive advantage lies.
Expert compliance support for IVDR labeling and translation
If you want pragmatic support for labeling and translation risk, we are here to help.
AD VERBUM works with IVD manufacturers navigating IVDR Article 10 obligations across all EU languages and risk classes. Our IVD localization experts combine ISO 13485-aligned quality management with an AI+HUMAN hybrid translation workflow: client Term Bases and Translation Memories are ingested first, our proprietary LLM-based LangOps System generates terminology-governed output, and certified SME linguists review every document for regulatory accuracy and contextual precision. QA is aligned to ISO 17100 and ISO 18587. All processing runs on EU-hosted, ISO 27001-certified infrastructure.
Whether you need label translation for a Class C IVD submission, EUDAMED consistency audits, or full multilingual IFU validation packages, our team delivers at 3x to 5x the speed of traditional workflows without compromising audit-readiness. Contact our team to discuss your IVDR labeling project.
Frequently asked questions
What is the core translation requirement in IVDR Article 10?
IVDR Article 10 requires manufacturers to provide all labeling in the official language(s) of each EU Member State where the device is sold, and the information must be legible, indelible, and easily understood by the intended user.
How does IVDR labeling compare to MDR?
IVDR labeling is stricter than MDR because of expanded notified body involvement, higher device reclassification rates, EUDAMED UDI-DI consistency obligations, and a stronger mandate for lay-user comprehension in patient-near devices.
What are the risks of using unvetted translators for IVD labeling?
Translation errors from unvetted translators can result in missing safety information, failed notified body reviews, competent authority-ordered recalls, or suspension of market access in specific Member States.
What is a best practice for validating IVD labeling translations?
Pair back-translation with structured user comprehension testing, particularly for self-test and lay-user devices, and document both steps with reviewer credentials so the full validation evidence is ready for notified body audit.
Recommended

